Duodenal Switch
Recent data shows the one anastomosis gastric bypass (formerly the mini-gastric bypass) is safer than the duodenal switch. While we are proud of our many years with the duodenal switch operation, we have now changed our focus to the one-anastomosis gastric bypass as the better alternative than the duodenal switch.
For those who underwent gastric sleeve surgery, and find they need a revision, we believe the data is clear that the one-anastomosis gastric bypass is our preferred option.
Dr. Simpson’s first Duodenal Switch operation was in 2001, and he was an early pioneer in bringing laparoscopic (minimally invasive surgery) to this type of operation. He did hundreds of these operations with great success, but was concerned about the malnutrition seen after the operation. While many patients didn’t mind taking extra vitamins, and enjoyed the weight loss, Dr. Simpson began to consider other operations instead.
The Duodenal Switch is an effective long-term operation for weight loss, but only makes up 2% of all weight loss operations in the United States because it requires a lot of technical skill to perform.
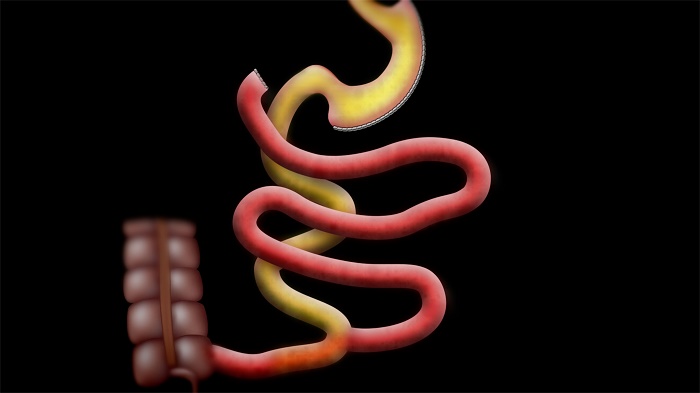
Part One – Vertical Sleeve Gastrectomy. Sometimes patients ask how much of the stomach we take out, though the important part is what is left. After the surgery, the stomach will look like a long tube (or a sleeve). A normal stomach can hold about 50 ounces, or 1.5 liters. After the Duodenal Switch surgery, the stomach holds about 4 to 8 ounces, or 0.12 to 0.24 liters. This enforces portion control. Over time, the stomach will enlarge a bit to accommodate a small to medium sized meal.
Some insurance companies do not cover weight loss (bariatric) surgery. If yours does not, and you wish to have weight loss surgery, we offer the most competitive cash prices in the US. While we cannot compete with Mexico cash prices, we can offer your surgery in a Center of Excellence, complete with post operative follow up using video or phone, and the knowledge that the people taking care of you meet the highest standards in the world. Oddly, our cash prices for the One-Anastomosis Gastric Bypass is the same as most prices for this procedure in Mexico. If you are interested, make an appointment today to talk to us in our Los Angeles adjacent practice, or email Dr. Simpson directly at simpson.office@gmail.com
Part Two – The second part of the Duodenal Switch looks like the RNY. Instead of connecting the stomach into the intestines, we connect the first portion of the duodenum. Rather than the entire small bowel having both food and digestive juices mixed, the end result will be half of that amount.
The standard DS we bypass most of the small bowel, and the common channel, or where the digestive juices end up with the food, is the last 125 cm of small bowel. This can lead to some issues with malabsorption, which is why our DS patients must commit to taking vitamins for the rest of their lives – especially those with ADEK in them. .
Why was the Duodenal Switch so Successful
We used to believe that one of the keys to successful weight loss after the Duodenal Switch is a muscle at the end of the stomach called the pylorus. It’s technically a muscular sphincter or a valve. It stays shut while food is in the stomach. When the pylorus muscle is closed, the stomach works as a hopper to digest food. Food stays in the stomach because this muscle is shut. The stomach churns away, adding acid and digestive enzymes until the food is the consistency of a thick shake. When the food reaches that consistency, it is ready to enter the small bowel. The pylorus then opens and this partially digested food goes into the duodenum (first part of the small bowel). If you drink liquids the pylorus opens and allows the liquids through quickly. Sometimes there is a bit of a delay, which means you should not drink fluids rapidly.
We now know this has little to do with the surgery.
With the gastric bypass, eating and drinking at the same time can cause issues as food is pushed through the stoma into the intestine too rapidly, leaving you feeling hungry. Many people can “eat around” a RNY gastric bypass. But not with the duodenal switch. With the Duodenal Switch surgery, you will simply fill up faster if you eat and drink at the same time. The pylorus doesn’t let food go past it – so with the Duodenal Switch you cannot overcome it by eating more, unless you stretch the stomach out. Our Camarillo weight loss surgery center is accepting patients now.
The second reason the Duodenal Switch was effective is that half of your small intestine is bypassed, which is far more than most other operations. The Duodenal Switch is more elegant than “restricting” food and causing “malabsorption.” It changes the regulation of several hormones that affect hunger, satiety, and appetite. It appears the Switch does this better than other operations, which is why the Duodenal Switch, and its cousin, the SADI, are amazing operations for weight loss for some individuals and great options for people who have had weight regain from gastric bypass. Sadly, too much was bypassed and some people suffered from severe malnutrition.
Who might benefit from the duodenal switch, or the SADI? We no longer offer this surgery for patients.
Instead, we feel the OAGB is a far superior operation, with the same weight loss but less risk of malabsorption.
Talk directly to Dr. Simpson and learn more about your options. Our practice is convenient to Santa Barbara, Malibu, and Ventura County.